- A nonunion is an arrest in the fracture repair process
- progressive evidence of non healing of a fracture of a bone
- a delayed union is generally defined as a failure to reach bony union by 6 months post-injury
- this also includes fractures that are taking longer than expected to heal (ie. distal radial fractures)
- large segmental defects
- should be considered functional non-unions
- Pathophysiology
- multifactorial
- most commonly, inadequate fracture stabilization and poor blood supply lead to nonunion
- infection
- eradication needs to occur along with the achieving fracture union
- smoking
- location
- scaphoid, distal tibia, base of the 5th metatarsal are at higher risk for nonunion because blood supply in these areas
- pattern
- segmental fractures and those with butterfly fragments
- increased risk of nonunion like because of compromise of the blood supply to the intercalary segment
- multifactorial
- Classification
- Types of nonunion
- septic nonunion
- pseudoarthrosis
- hypertrophic nonunion
- atrophic nonunion
- caused by inadequate immobilization and inadequate blood supply
- oligotrophic nonunion
- produced by inadequate reduction with fracture fragment displacement
- Types of nonunion
- Presentation
- Symptoms
- important to discern injury mechanisms, non operative interventions, baseline metabolic, nutritional or immunologic statuses and use of NSAIDs and/or nicotine containing products
- assess pain levels with axial loading of involved extremity
- Physical exam
- important to complete a thorough neurovascular exam, including the status of the soft tissue envelope
- assess mobility of the nonunion
- assess extremity for the presence of deformity
- Symptoms
- Imaging
- Radiographs
- plain radiographs are the cornerstone for evaluation of fracture healing; four views should be included
- full length weight bearing films should obtained if a limb length discrepancy is present
- CT
- if the status of union is in question, a CT scan should be obtained; hardware artifact may limit utility of the CT scan
- Radiographs
- Treatment
- Nonoperative
- fracture brace immobilization
- bone stimulators
- contraindications include synovial pseudoarthroses, nonunions that move and greater than 1 cm between fracture ends
- Operative
- infected nonunion
- often associated with pseudoarthrosis
- chance of fracture healing is low if the infection isn’t eradicated
- a staged approach is often important
- modalities
- need to remove all infected/devitalized soft tissue
- use antibiotic beads, and VAC dressings to manage the wound
- with significant bone loss, bone transport may be an option
- muscle flaps can be critical in wound management with soft tissue loss
- need to remove all infected/devitalized soft tissue
- pseudoarthrosis
- may be found in association with infection
- the joint capsule may be encountered with operative exposure
- modalities
- removal of atrophic, non-viable bone ends
- internal fixation with mechanical stability
- maintenance of viable soft tissue envelope
- hypertrophic nonunions
- often have biologically viable bone ends
- the issue with fixation, not the biology
- modalities
- internal fixation with the application of appropriate mechanical stability
- oligotrophic nonunions
- often have biologically viable bone ends
- may require biological stimulation
- modalities
- internal fixation
- atrophic nonunions
- often have dysvascular bone ends
- mobile
- modalities
- need to ensure biologically viable bony ends are apposed
- fixation needs to be mechanically stable
- bone grafting
- autologous iliac crest (osteoinductive) is the gold standard
- BMPs
- osteoconductive agents (ie. crushed cancellous chips, DBM)
- establishment of healthy soft tissue flap/envelope
- infected nonunion
- Nonoperative
Cases ( Before and After )
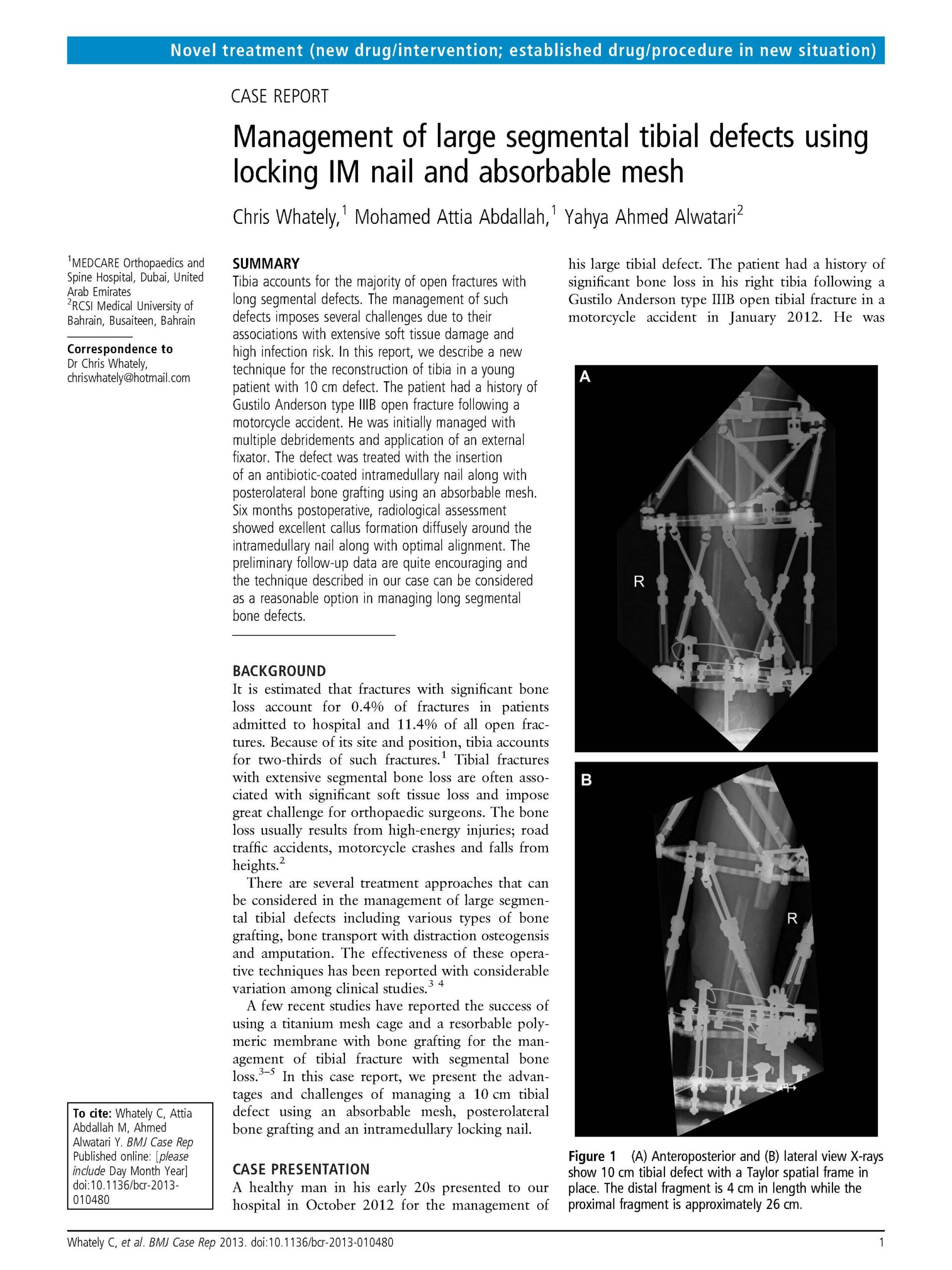
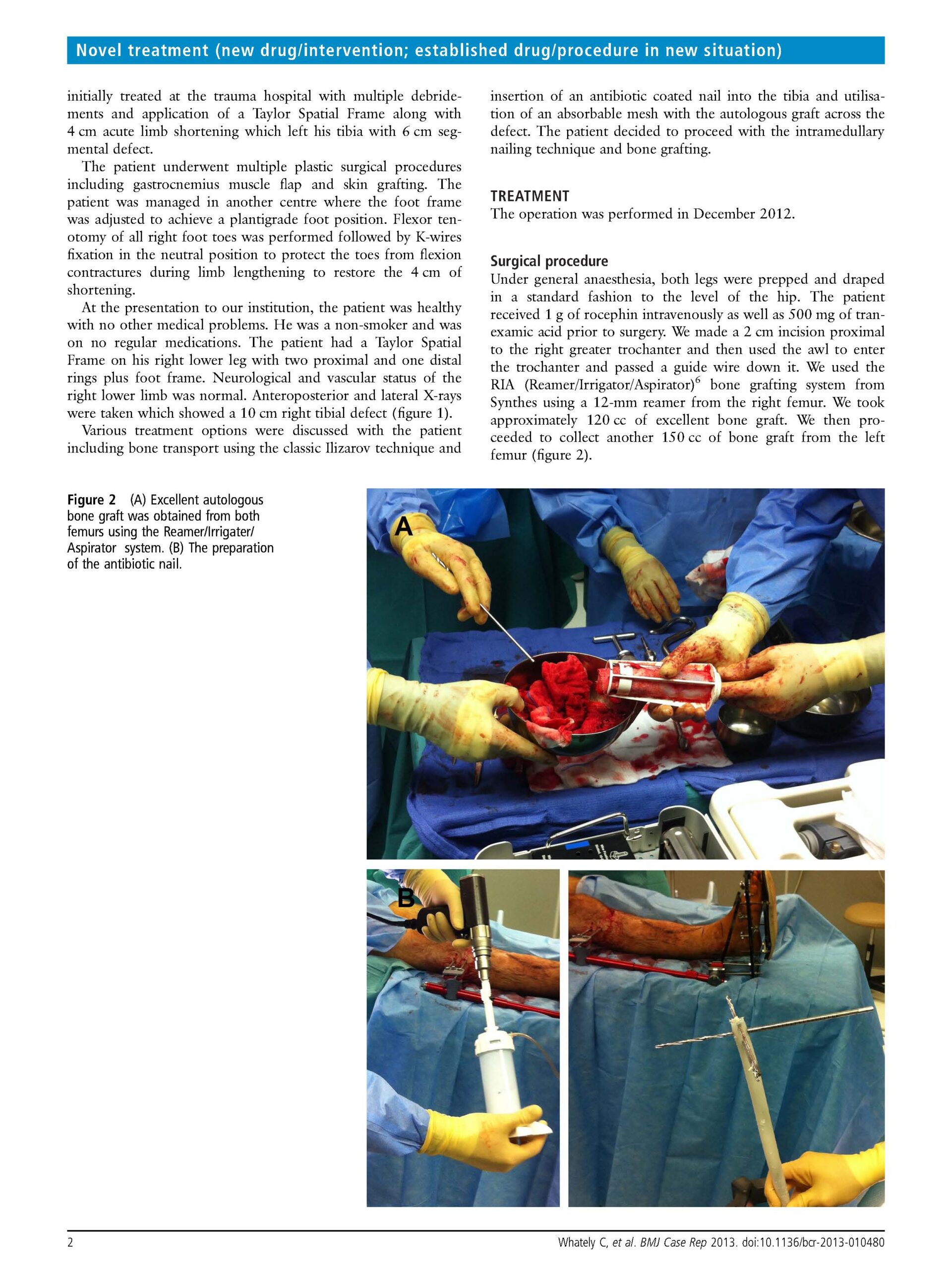
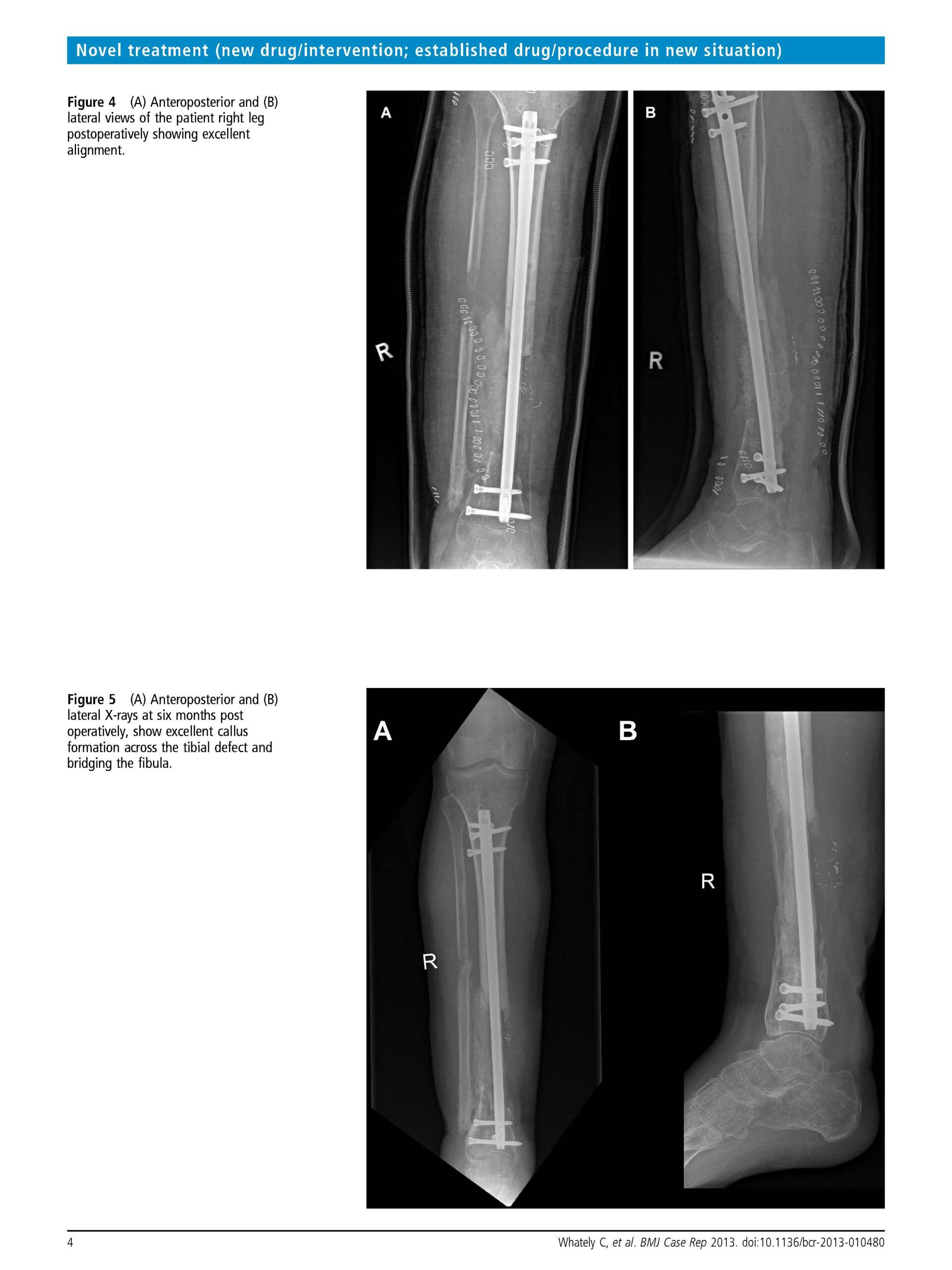
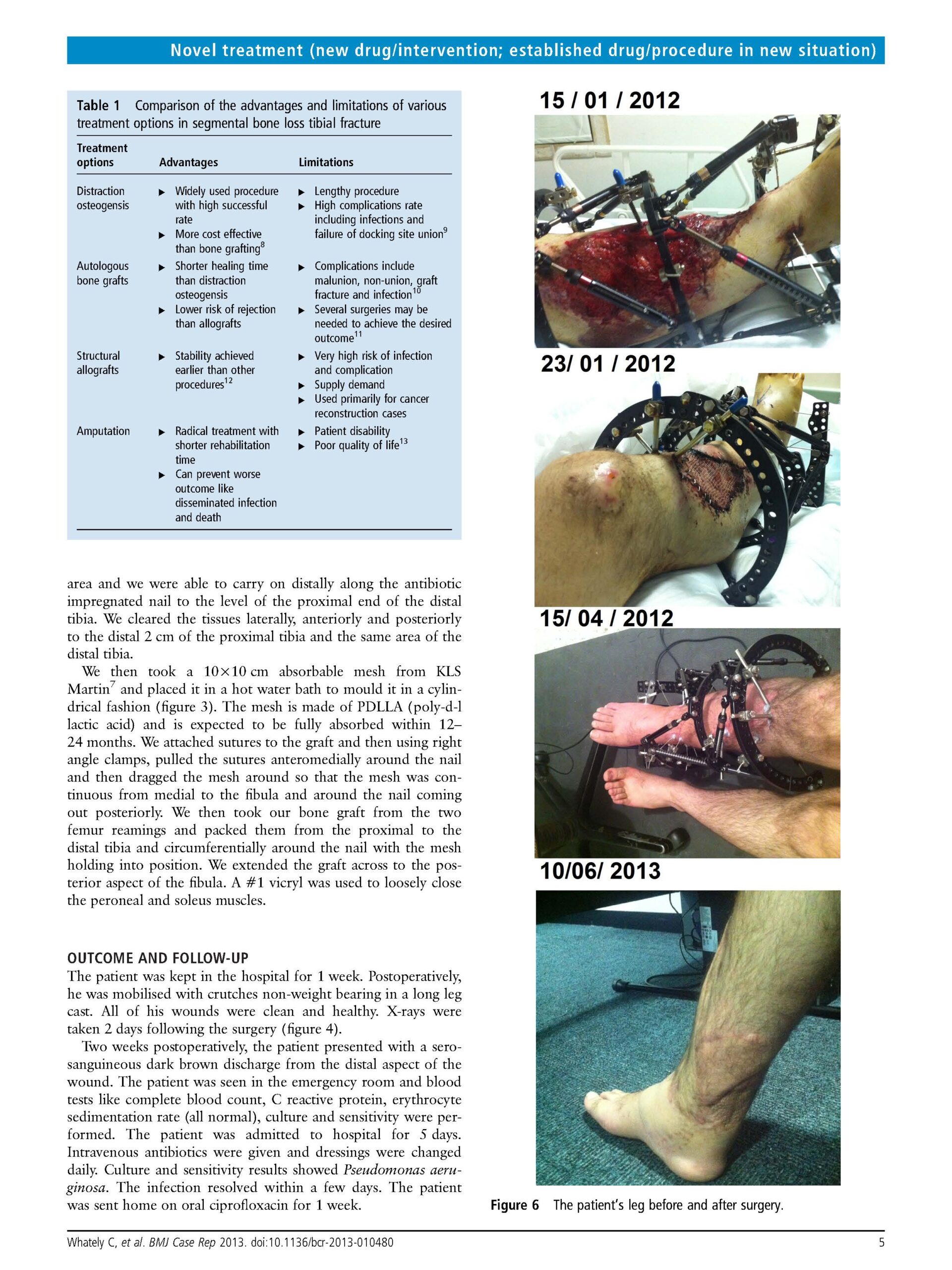
Case 1 - Management of large segmental tibial defects using locking IM nail and absorbable mesh


Case 2







