Limb lengthening and reconstruction techniques can be used to replace missing bone and to lengthen and/or straighten deformed bone segments. These procedures may be performed in both children and adults who have limb length discrepancies due to birth defects, disease, or injury.
The limb lengthening and deformity correction process works on the principle of distraction osteogenesis. This is a revolutionary concept, reversing the long-held belief that bone could not be regenerated. With this process, a bone that has been cut during surgery is gradually distracted (pulled apart), leading to new bone formation (osteogenesis) at the site of the lengthening. In this way, bone segments can be lengthened by 15 to 100% of their original length.
Indications
- Leg Length Discrepancy
- Post-Traumatic Bone Deformities
- Nonunions
- Malunions
- Bone Loss
- Joint Contractures
- Osteomyelitis
Leg Length Discrepancy
Leg length discrepancy (LLD) results from congenital, developmental, posttraumatic, or post-surgical causes.
Posttraumatic LLD occurs after fractures when bones heal in a shortened position.
Treatment goals are correction of LLD with associated deformity while preserving function of muscles and joints and restoring normal alignment of the limb.
Post-Traumatic Bone Deformities
Posttraumatic bone deformities are fractures that heal in a displaced, angulated, rotated, or shortened position.
Non-Healing Fractures (Nonunions) And Malunions
Fractures that do not heal result in nonunions. These may be associated with limb length discrepancy, infection, and stiff joints.
Fractures can heal in an incorrect position with shortening, angulation or rotation. This is called a malunion.
Bone Loss From Tumour, Trauma Or Infection
Tumour, trauma, and infection can all lead to bone loss due to either the injury or resection. Bone loss may be manifested as a bone defect or as limb length discrepancy or both.
Joint Contractures
Joints may be limited in their movement from tight muscles or capsule or from scarring in the joint.
Bone Infection (Osteomyelitis)
Bone infection may be a result of fracture or blood borne infection (usually occur during childhood). Usually the only way to effectively eradicate established bone infection is to
resect the abnormal bone and this can result in a bone defect that needs to be reconstructed using the Ilizarov technique.
The Process
Phase 1: Consultation
The initial assessment involves detailed history examination and review of previous x-rays. Specialized x-rays are usually required to complete the assessment. The initial assessment and discussion often takes an hour.
If surgical treatment is considered appropriate, all aspects of the procedure are discussed with the patient. The patient is encouraged to consider the information and a follow up appointment is made to answer any further questions and make definitive treatment plans.
It is extremely important that the patient and the surgeon have a clear understanding of the goals of surgery. It is important the patient understands what can realistically be achieved by the surgery and the potential complications both common and minor and rare but serious.
Phase 2: Surgery
The surgeon in preparation for each surgery preconstructs a customized apparatus. Using wires or pins, the apparatus is surgically attached to the affected limb. Surgery is usually performed percutaneously through small incisions. Special care is taken to minimize injury to the bone and surrounding soft tissue, nerves and blood vessels when making specialized bone cuts.
Phase 3: Postoperative Treatment And Rehabilitation
Adjustment Phase
Generally, patients remain in the hospital for 3 to 7 days before they are discharged home. A more complex procedure may require a longer inpatient stay.
The actual lengthening or straightening of the limb begins 1-2 weeks after surgery. At that time, adjustments are made to the apparatus usually four times a day. Detailed instructions are provided to the patient to ensure they fully understand what is required.
The bone ends are separated at a rate of 1 mm per day.
Muscles do not lengthen as easily as bone and therefore physiotherapy may be an important part of the treatment to maintain joint range of motion and prevent contractures. A joint at risk may be included in the frame to prevent contractures that would otherwise occur.
Swimming and showering are allowed with the apparatus in place once initial wound healing has occurred at 5-7 days postoperatively.
During the adjustment phase the patient is followed up in the rooms every two weeks with clinical examination and x-rays. A close scrutiny is maintained to identify any complications early.
Phase 3: Postoperative Treatment And Rehabilitation
Adjustment Phase
Generally, patients remain in the hospital for 3 to 7 days before they are discharged home. A more complex procedure may require a longer inpatient stay.
The actual lengthening or straightening of the limb begins 1-2 weeks after surgery. At that time, adjustments are made to the apparatus usually four times a day. Detailed instructions are provided to the patient to ensure they fully understand what is required.
The bone ends are separated at a rate of 1 mm per day.
Muscles do not lengthen as easily as bone and therefore physiotherapy may be an important part of the treatment to maintain joint range of motion and prevent contractures. A joint at risk may be included in the frame to prevent contractures that would otherwise occur.
Swimming and showering are allowed with the apparatus in place once initial wound healing has occurred at 5-7 days postoperatively.
During the adjustment phase, the patient is followed up in the rooms every two weeks with clinical examination and x-rays. Close scrutiny is maintained to identify any complications early.
Phase 4: Restoration of endosteal and periosteal blood vessels
Distraction phase– 1mm/day until the desired length is achieved.
Consolidation phase allows for intramembraneous ossification and recanalization of new bone.
Consolidation Phase (Bone Hardening)
After the desired length has been achieved and the limb has been straightened, no further adjustments are made. The apparatus is left in place to allow the new bone to harden and mature. Once the new bone is judged to be sufficiently strong, the frame is removed under a short general anesthetic. A cast or brace may be applied for an additional month or two for further protection. The new bone tissue assumes all the qualities and strength of normal bone with time.
During the adjustment phase, the patient is seen every month.
Follow-Up
With close follow up if a problem is arising then it can be picked up early and can usually be treated without affecting the final outcome.
All the necessary surgeries are anticipated and communicated to the patient before treatment commences but sometimes an unscheduled operation is required to correct a problem. When the desired correction is achieved the frame is locked down and the consolidation phase begins. The patient is seen on a monthly basis with x-rays and examination.
I am very conservative regarding when to remove the frame. This is to minimize the risk of deformation of the regenerate or fracture after frame removal, which can be a devastating complication. When it is thought that it is time to remove the frame then it is completely loosened so that it is not assisting in weight-bearing and the patient is encouraged to fully weight bear for two weeks. If this can be achieved without any loss of correction then the frame removal is scheduled. If there is a loss of position then usually this can be corrected by frame adjustment on an outpatient basis thereby avoiding needing further surgery.
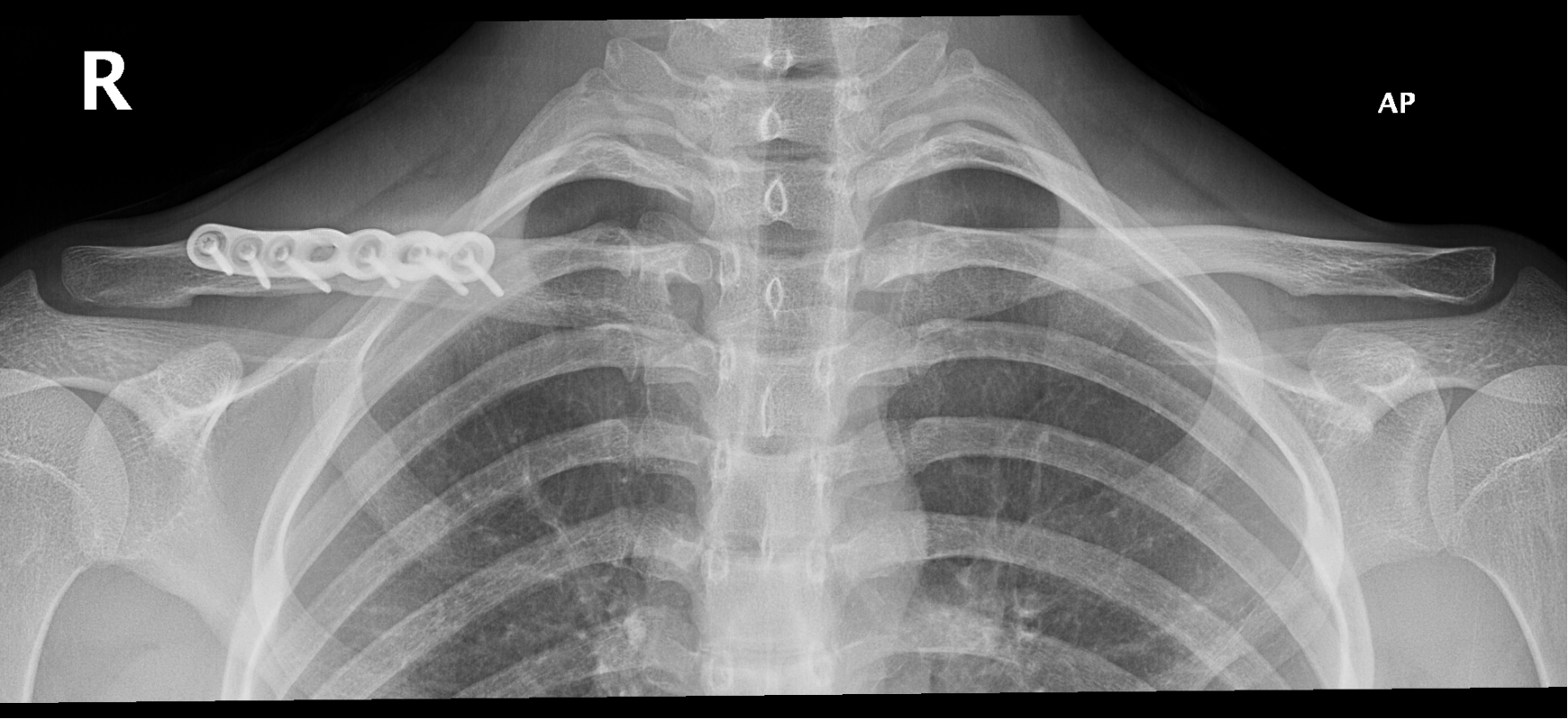
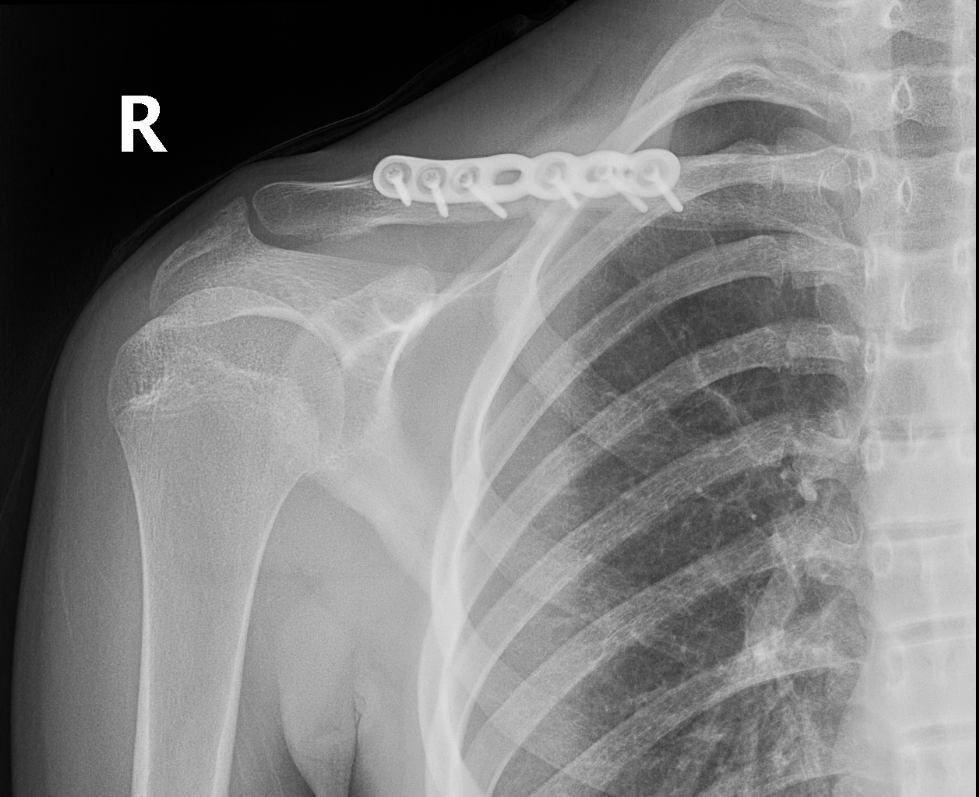
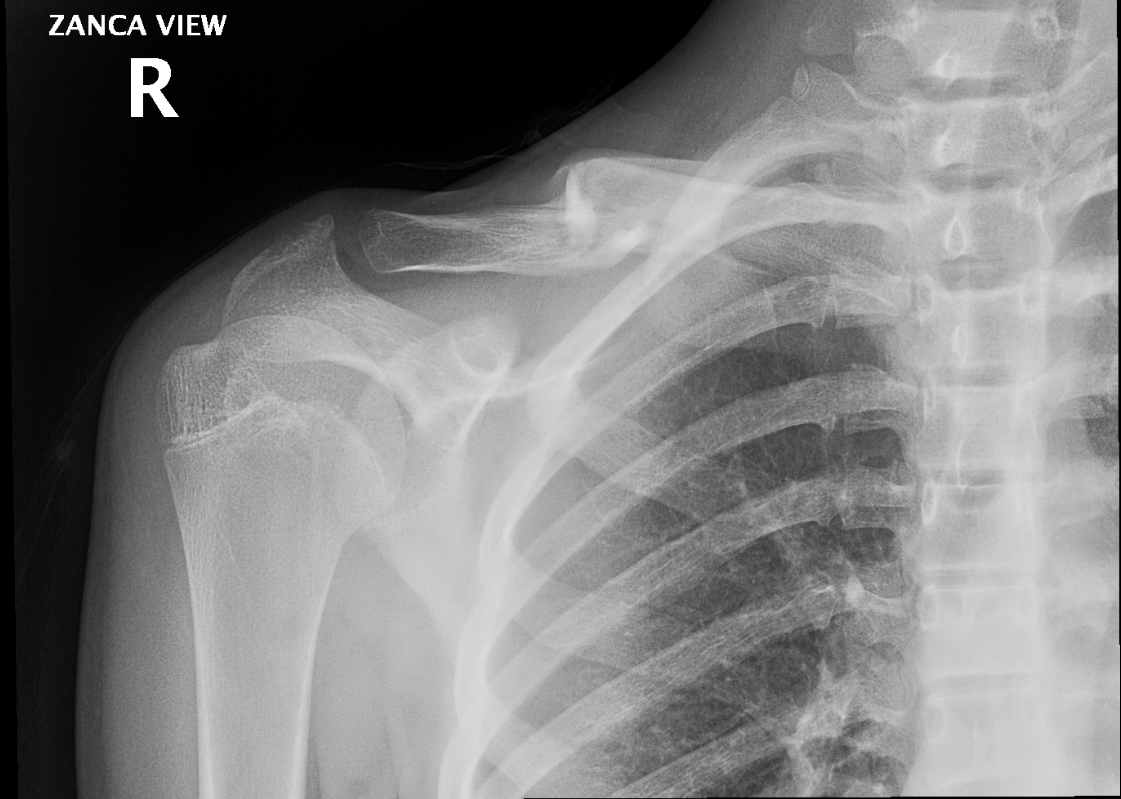
Cases ( Before and After )
Case 1








Case 2

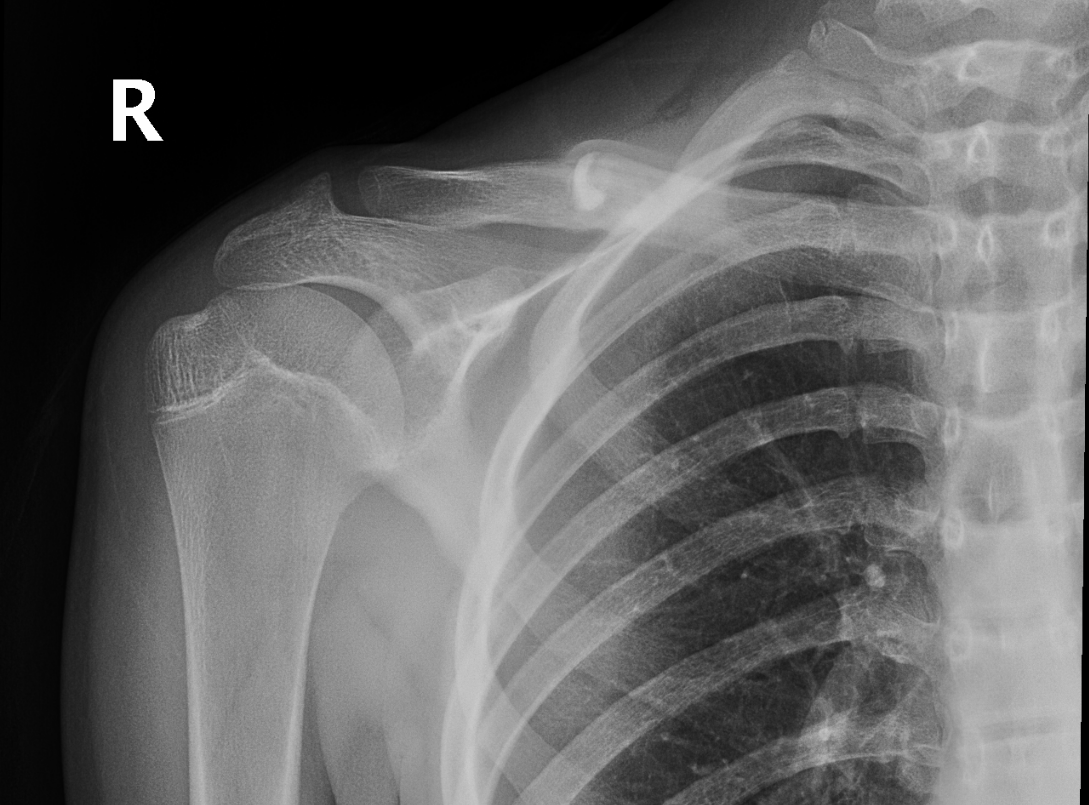
Case 3




Case 4




Case 5



Case 6


Case 7





